
A 23-year-old girl presents to Outpatient Department with complaints of gradually
progressive shortness of breath and painful nodular reddish rash over both shins.
Chest X-ray shows hilar fullness, tracheobronchial biopsy findings including large
epithelioid cells, occasional giant cells and no areas of necrosis.
a) Write down two differential diagnoses.
b) What is your treatment plan for the likely diagnosis?
Sarcoidosis is a multisystem disorder, characterized by non-caseating epithelioid granulomas; it is more common in colder parts of Northern Europe.
The etiology is unknown, although atypical mycobacteria, viruses and genetic factors have been proposed.
Clinical Features
Any organ may be affected but 90% of cases affect the lungs.
Most frequently involved sites.
- lymph glands
- liver
- spleen
- skin
- eyes
- parotid glands
- phalangeal bones
Löfgren’s syndrome – erythema nodosum, peripheral arthropathy, uveitis, bilateral hilar lymphadenopathy (BHL), lethargy and occasionally fever.
Investigations
- lymphopenia is characteristic
- Liver Function Tests: may be mildly deranged.
- Ca2+ may be elevated.
- Serum ACE may provide a non-specific marker of disease activity.
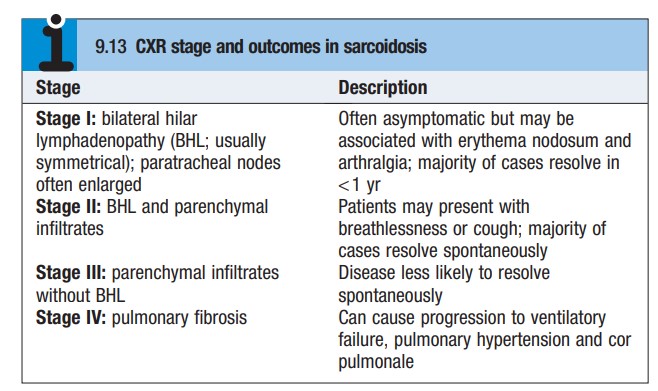
- CXR: used to stage sarcoid (see below)
- HRCT: characteristic appearances include reticulonodular opacities that follow a peri lymphatic distribution centered on broncho vascular bundles and the subpleural areas.
- Pulmonary function may show restriction and desaturation on exercise.
- Bronchoscopy: may demonstrate a ‘cobblestone’ appearance of the mucosa
- Bronchial and transbronchial biopsies usually show non-caseating granulomas.
- The occurrence of erythema nodosum in patients in the second to third decades with BHL on CXR is often sufficient for a confident diagnosis
Management
The majority of patients enjoy spontaneous remission and, if there is no evidence of organ damage, it is appropriate to withhold therapy for 6 months. Patients who present with acute illness and erythema nodosum may require NSAIDs and, if systemically unwell, a short course of corticosteroids. Systemic corticosteroids are also indicated in the presence of hypercalcemia, pulmonary function impairment and renal impairment. Uveitis responds to topical steroids. In patients with severe disease, both methotrexate and azathioprine have been used successfully and selected patients with severe disease may be referred for single lung transplantation.
A 23-year-old girl presents to Outpatient Department with complaints of gradually
progressive shortness of breath and painful nodular reddish rash over both shins.
Chest X-ray shows hilar fullness, tracheobronchial biopsy findings including large
epithelioid cells, occasional giant cells and no areas of necrosis.
a) Write down two differential diagnoses.
b) What is your treatment plan for the likely diagnosis?
Reference: Davidson’s Principle and practices of Medicine and Davidson’s Essential of medicine